Pulse Pressure Variation 101: A Beginner’s Guide to Hemodynamic Monitoring
Hemodynamic monitoring is the unsung hero of critical care medicine, providing real-time insights into a patient’s cardiovascular status to guide life-saving interventions. For beginners stepping into the world of intensive care units (ICUs) or operating rooms, terms like cardiac output, preload, and fluid responsiveness can feel overwhelming. At the heart of this—pun intended—is Pulse Pressure Variation (PPV), a dynamic tool that helps clinicians determine if a patient will benefit from fluid therapy without the guesswork.
Imagine a patient in septic shock: their blood pressure is low, tissues are starving for oxygen, and the knee-jerk reaction might be to pump in fluids. But overload them, and you risk pulmonary edema or worsening organ failure. PPV steps in as a reliable predictor of “fluid responsiveness”—whether giving 250-500 ml of fluid will boost stroke volume by at least 10-15%. This beginner’s guide breaks down PPV from the ground up: what it is, why it works, how to use it, and where it’s headed. By the end, you’ll see why Pulse Pressure Variation is transforming hemodynamic monitoring from an art into a science.
What is Pulse Pressure Variation?
Pulse Pressure Variation, often abbreviated as PPV, is a simple yet powerful metric derived from arterial blood pressure waveforms. It measures the beat-to-beat fluctuations in pulse pressure—the difference between systolic (top number) and diastolic (bottom number) blood pressure—caused by the mechanical breaths of a ventilator.
In essence, PPV quantifies how much the heart’s output swings with each breath in a mechanically ventilated patient. These swings happen because positive pressure ventilation temporarily squeezes the heart and blood vessels, altering blood flow. When PPV is high, it signals that the heart is preload-dependent, meaning more fluid could help fill it up and improve output. Low PPV? The heart’s already adequately filled, and extra fluids might just cause harm.
For newcomers, think of PPV as a traffic light for fluids: green for “go ahead,” red for “stop,” and yellow for “proceed with caution.” It’s especially useful in sedated, paralyzed patients on controlled ventilation, where traditional static measures like central venous pressure (CVP) often mislead.
The Physiology Behind Pulse Pressure Variation
To grasp PPV, you need a quick physiology primer. The heart follows the Frank-Starling law: stretch it more (with preload, or blood volume returning to it), and it pumps stronger—up to a point. Plot this as a curve: steep at low preload (room for improvement), flat at high preload (no gains from more stretch).
Enter mechanical ventilation. During inspiration, the ventilator pushes air into the lungs, raising pressure in the chest. This compresses the vena cava, reducing blood return to the right ventricle and kinking left ventricular filling. The result? A temporary drop in stroke volume and pulse pressure. Expiration reverses it, causing a rebound.
In fluid-responsive patients (on the steep curve part), these swings are exaggerated—Pulse Pressure Variation amplifies. In non-responders (flat curve), they’re minimal. This respiratory-cardiac interplay makes PPV a dynamic window into preload status, far superior to snapshots like CVP, which ignore ventilation’s effects.
Tidal volume matters here: breaths of 8 ml/kg or more create stronger pressure changes, making PPV reliable. In protective strategies for ARDS (acute respiratory distress syndrome), smaller breaths (6 ml/kg) can mute the signal, but tweaks like temporary volume increases help.
How to Measure Pulse Pressure Variation
Measuring PPV is straightforward with modern monitors, but it starts with an arterial line—a catheter in an artery (usually radial) for continuous pressure readings. No arterial line? PPV isn’t feasible, though non-invasive cuffs are emerging but less accurate.
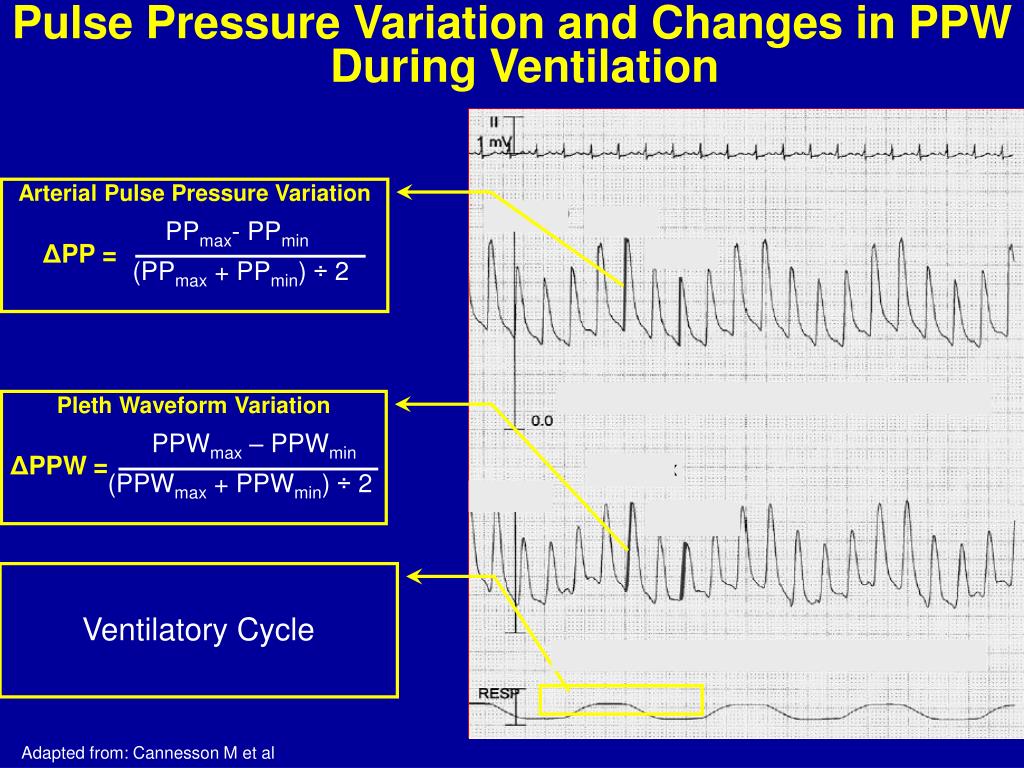
The calculation is automated on devices like Philips IntelliVue or GE CARESCAPE: over a full respiratory cycle (inspiration to inspiration), find the maximum (PP_max) and minimum (PP_min) pulse pressures. Then:
PPV (%) = [(PP_max – PP_min) / ((PP_max + PP_min) / 2)] × 100
This “mean” in the denominator averages the extremes for a cycle. Aim for at least three cycles to smooth noise. Quality matters—dampened waveforms from air bubbles or kinks skew results.
For beginners: Set your monitor to display PPV (often under “advanced hemodynamics”). Ensure sinus rhythm, no arrhythmias, and controlled ventilation. If tidal volume’s low, try a “tidal volume challenge”: bump it to 8 ml/kg for 1-2 minutes and recheck.
Interpreting PPV Values
Reading PPV is like checking a weather app—thresholds guide action. A PPV greater than 13% screams fluid responsiveness: give that bolus and watch output rise. Below 9%? Hold off; the patient’s likely optimized. The 9-13% “gray zone” is trickier—about 40% of cases—warranting extras like passive leg raising (PLR) to simulate a fluid load without committing.
Context is king. In sepsis or hypovolemia, high PPV aligns with distributive shock’s low preload. But in heart failure, it might falsely elevate due to stiff ventricles. Always pair with clinical signs: lactate levels, urine output, skin mottling.
Recent data refines this: in low-effort spontaneous breathing (e.g., airway pressure <1.5 cmH₂O), PPV still predicts responsiveness, opening doors beyond full paralysis.
Clinical Applications of Pulse Pressure Variation
PPV shines in high-stakes scenarios. In the OR during major abdominal surgery, it tailors intraoperative fluids, cutting complications like ileus or acute kidney injury. Post-op in the ICU, it streamlines sepsis bundles: fluid-challenge only if PPV >13%, aligning with Surviving Sepsis guidelines.
For beginners, start with goal-directed therapy (GDT): Use PPV to hit targets like mean arterial pressure >65 mmHg without overload. Studies show GDT with PPV shortens ICU stays by a day and trims costs. It’s also handy in neurocritical care, balancing cerebral perfusion sans edema, or trauma, where occult hypovolemia hides.
Beyond PPV, integrate with stroke volume variation (SVV) or pleth variability index (PVI) from pulse oximetry for a fuller picture—non-invasive backups when lines aren’t placed.
Advantages and Limitations of PPV
Why love Pulse Pressure Variation? It’s continuous, objective, and beats static params in trials—sensitivity around 90% for responsiveness. No extra tests needed beyond the vent and art line, and its negative predictive value (ruling out non-responders) prevents over-resuscitation, a top ICU foe.
But it’s no panacea. PPV demands mechanical ventilation sans patient effort—spontaneous breaths muddy the waves. Low tidal volumes in ARDS blunt it; high rates (>30/min) wash it out. Arrhythmias (AFib), valve issues, abdominal hypertension, or open chests invalidate readings. In right-heart failure, ventilation’s squeeze overemphasizes variations, fooling you into fluids that worsen pulmonary hypertension.
For novices: Always verify assumptions. If in doubt, cross-check with PLR or echo.
Emerging Trends in PPV Monitoring
As of 2025, PPV’s evolving. Machine learning refines gray-zone calls, blending it with AI-driven waveforms for 95% accuracy. Dynamic arterial elastance (PPV/SVV ratio >0.84) predicts pressure responses to vasopressors, per fresh studies. Tidal volume challenges and mini-boluses (100 ml) rescue low-volume cases, while PLR-induced PPV shifts forecast responsiveness even better in meta-analyses.
Non-invasive frontiers: Finger-cuff tech like Clearsight approximates PPV without lines. In spontaneously breathing patients with assist, low-effort thresholds expand use to weaning phases. Look for hybrid tools merging PPV with ultrasound for bedside precision medicine.
Conclusion
Pulse Pressure Variation demystifies hemodynamic monitoring, turning ventilator breaths into actionable intel for fluid smarts. From its Frank-Starling roots to 2025’s AI boosts, PPV empowers beginners and vets alike to optimize therapy, dodge pitfalls, and boost survival odds.
Mastering it isn’t rote—it’s rhythmic, syncing breath, beat, and brain. As you monitor your first PPV trace, remember: it’s not just a number; it’s a narrative of resilience, guiding patients from instability to steady sails. Dive in, interpret wisely, and watch hemodynamics unfold.